
Read the document
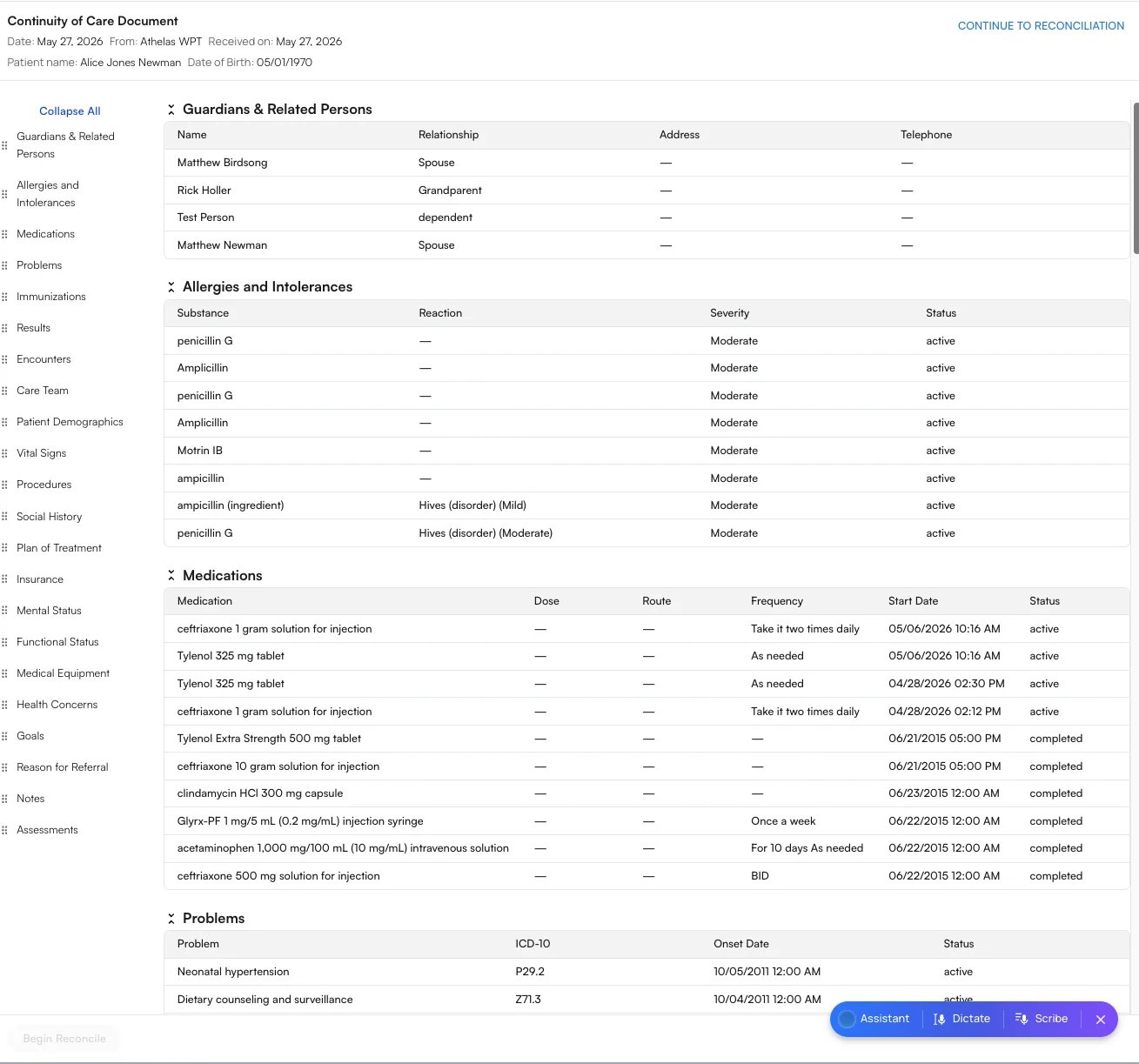
The document opens as a Continuity of Care Document, showing the patient’s name, date of birth, the sending site, and the date received. Its contents are organized into the standard C-CDA clinical sections—for example Guardians & Related Persons, Allergies and Intolerances, Medications, Problems, Immunizations, Results, and more. You also have two ways to keep the source data:- Additional Files — Files attached during the transition of care (for example, an X-ray report or urinalysis). Clicking a file downloads it so you can open it in your preferred viewer.
- Download XML — Downloads the exact XML document that was sent to you.
Understanding the C-CDA sections
A C-CDA is organized into standard clinical sections defined by the C-CDA / USCDI standard. Each section is a self-contained part of the patient’s chart—allergies, medications, problems, and so on—and is shown in Air as a labeled table. Not every document includes every section: a section only appears when the sending system populated it, so a given C-CDA may show only a handful of the sections below. The table below explains every section you may encounter, what clinical information it holds, and the columns you’ll see inside it.When you reconcile a document, the categories you actively incorporate into the chart—per ONC criterion §170.315(b)(2)—are Medications, Allergies and Intolerances, and Problems. The remaining sections are read-only clinical context that travels with the document. See Viewing and Reconciling Incoming C-CDAs.
Customize your view
To make long documents easier to read:- Every section is collapsible. Use Collapse All to collapse them at once.
- Rearrange sections by dragging them using the handles in the left sidebar.
Your view preferences are saved across all notes, not just the document you’re looking at. If you collapse or rearrange the sections while viewing Alice Newman’s document, the next patient you open—say, Jeremy Bates—will be laid out exactly the same way. You set up your view once and it carries over to every patient, so there’s no need to switch it back each time.
FAQ
Can I keep a copy of the original document?
Can I keep a copy of the original document?
Yes. Use Download XML to save the exact document that was sent to you, and open any attachments from the Additional Files menu.
Do my collapse and section-order preferences apply to other patients?
Do my collapse and section-order preferences apply to other patients?
Yes. View preferences are saved across all notes, so the layout you set on one patient’s document carries over to every patient you open next—no need to rearrange each time.